FEBRUARY BIMONTHLY ASSESMENT
FEBRUARY BIMONTHLY ASSESMENT
February 18, 2021
Case:1
50 year man, he presented with the complaints of
Frequently walking into objects along with frequent falls since 1.5 years
Drooping of eyelids since 1.5 years
Involuntary movements of hands since 1.5 years
Talking to self since 1.5 years
More here:
Case presentation links:
https://youtu.be/kMrD662wRIQ
a). What is the problem representation of this patient and what is the anatomical localization for his current problem based on the clinical findings?
Problem representation:
Problem to be attended:
Diabetes,Seizures,Frequent falls,Ptosis,Tremors,self talk
Anatomical localization:
Brain
B/l ptosis :there is no loss of frowning which may indicate weakness of levator palbebral superioris
b) What is the etiology of the current problem and how would you as a member of the treating team arrive at a diagnosis? Please chart out the sequence of events timeline between the manifestations of each of his problems and current outcomes.
Etiology:
Progressive supranuclear palsy.
etiology is likely due to accumulation of 'tau' protein in brain
Sequence of events:
1.Seizures 10 years back
2.Type 2DM 2 years back
3.Sudden blurring of vision while riding bike met with RTA -- fracture in left leg for which he was operated
Frequently walking into objects along with frequent falls,drooping of eyelids,I,Involuntarymovements of hands,Talking to self 1.5 years back
Stoppedalcohol & tobacco consumption 1 year back.Non productive cough 8 months back.Non healing ulcer at surgical site 7 months back
For 1 week - diagnosed as PSP & discharged with SYNDOPA 110 MG & QUETIAPINE
5 days later patient presented to casualty in a state of unresponsiveness with GCS: 3/15 with H/o 2-3 episodes vomiting.
Another 2 episodes of generalized tonic seizures in casualty - treated with levipil
Suddenly his saturations & heart rate dropped with no peripheral pulsations and patient was intubated - CPR done and was resuscitated.
He's on mechanical ventilator on cpap now
c) What is the efficacy of each of the drugs listed in his current treatment plan Quetiapine-For psychosis in PSP
SYNDOPA-helps parkinson as well as psp according to ncbi
Case:2
Patient was apparently asymptomatic 2 years back then he developed weakness in the right upper and lower limb, loss of speech.
More here:
Case presentation links:
https://youtu.be/7rnTdy9ktQw
a). What is the problem representation of this patient and what is the anatomical localization for his current problem based on the clinical findings?
Problem presentation:
60 year old male non diabetic & non hypertensive who had a history of CVA 2 years back now presented with c/o SOB,pedal edema,decreased urine output & generalized weakness since 2 months.
Anatomical localization:
Heart - HFrEF secondary to CAD with EF 36 PERCENT
b) What is the etiology of the current problem and how would you as a member of the treating team arrive at a diagnosis? Please chart out the sequence of events timeline between the manifestations of each of his problems and current outcomes.
Etiology:
Coronary artery disease
Ecg shows
1.pathological Q waves from v1 to v6
2.poor R wave progression
suggest a CAD probably involving LAD territory
Sequence of events:
CVA -2 years back
and
SOB, pedal edema, decreased urine output & generalized weakness since 2months
and
Treated with diuretics(aldosterone antagonist) and beta blockers ,ARB
With salt and Fluid restriction.
Outcome: Symptomatically improved and discharged
c) What is the efficacy of each of the drugs listed in his current treatment plan
Salt and fluid restriction
https://pubmed.ncbi.nlm.nih.gov/23787719/#:~:text=Conclusion%3A%20Individualized%20salt%20and%20fluid,Quality%20of%20life%3B%20Salt%20restriction.
Ninety-seven stable patients in NYHA class II-IV, on optimal medication, with previous signs of fluid retention, treated with either >40 mg (NYHA III-IV) or >80 mg (NYHA II-IV) of furosemide daily were randomized to either individualized salt and fluid restriction or information given by the nurse-led heart failure clinics, e.g. be aware not to drink too much and use salt with caution, and followed for 12 weeks. Fluid was restricted to 1.5 L and salt to 5 g daily, and individualized dietary advice and support was given.
Results After 12 weeks, significantly more patients in the intervention than in the control group improved on the composite endpoint (51% vs. 16%; P < 0.001), mostly owing to improved NYHA class and leg oedema. No negative effects were seen on thirst, appetite, or QoL
Benfomet as thiamine replacement in alcoholic patients
Case:3
52 year old male , shopkeeper by profession complains of SOB, cough ,decrease sleep and appetite since 10 days and developed severe hyponatremia soon after admission.
Morehere:
Case presentation video:
https://youtu.be/40OoVEQBgS4
a) What is the problem representation of this patient and what is the anatomical localization for his current problem based on the clinical findings?
Problem representation:
SOB,
cough,
decreased sleep&appetite
Diabetes
Hypertension
Anemia
Anatomical localization:
Anemia - Nutritional(iron and B12 deficiency)
Hyponatremia -SIADH or dilutional
b) What is the etiology of the current problem and how would you as a member of the treating team arrive at a diagnosis? Please chart out the sequence of events timeline between the manifestations of each of his problems and current outcomes.
Etiology:
Dimorphic anemia may be secondary to ? Nutritional
Hyponatremia secondary to free fluid (dilutional) or poor sugar control (hyperglycemia)
Sequence of events:
Type 2 DM & HTN since 1 year
And
SOB,Cough
Decreased sleep and appetite since 10 days
Diagnosed with hyponatremia
Treated conservatively & discharged
c) What is the efficacy of each of the drugs listed in his current treatment plan especially for his hyponatremia? What is the efficacy of Vaptans over placebo? Can one give both 3% sodium as well as vaptan to the same patient?
Can be given if it is SIADH tolvaptan can be given.
3percent NS may not be necessary because sodium levels here are 131 near to normal lower limit,no need of correction acutely.
4) Please mention your individual learning experience from this month
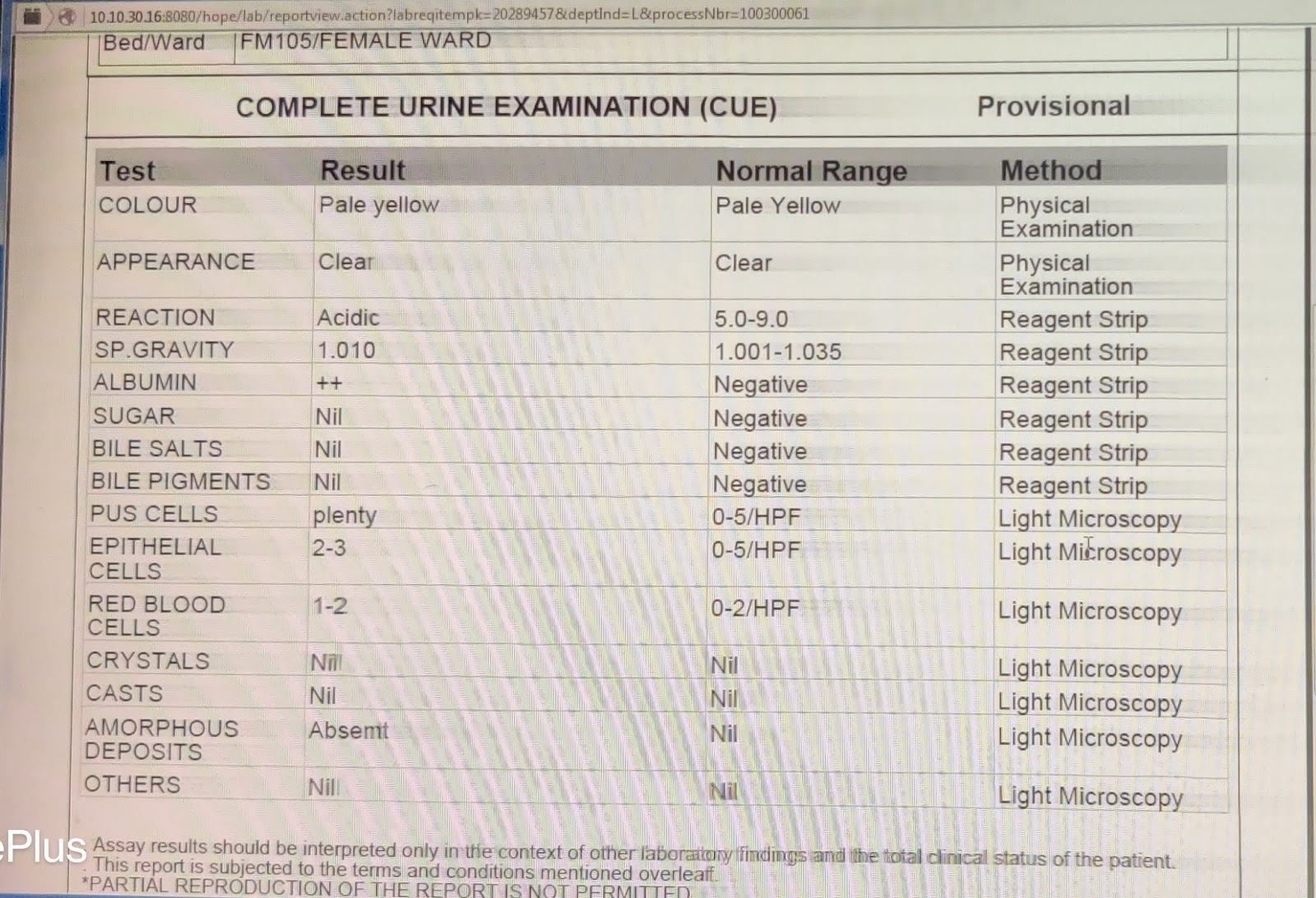
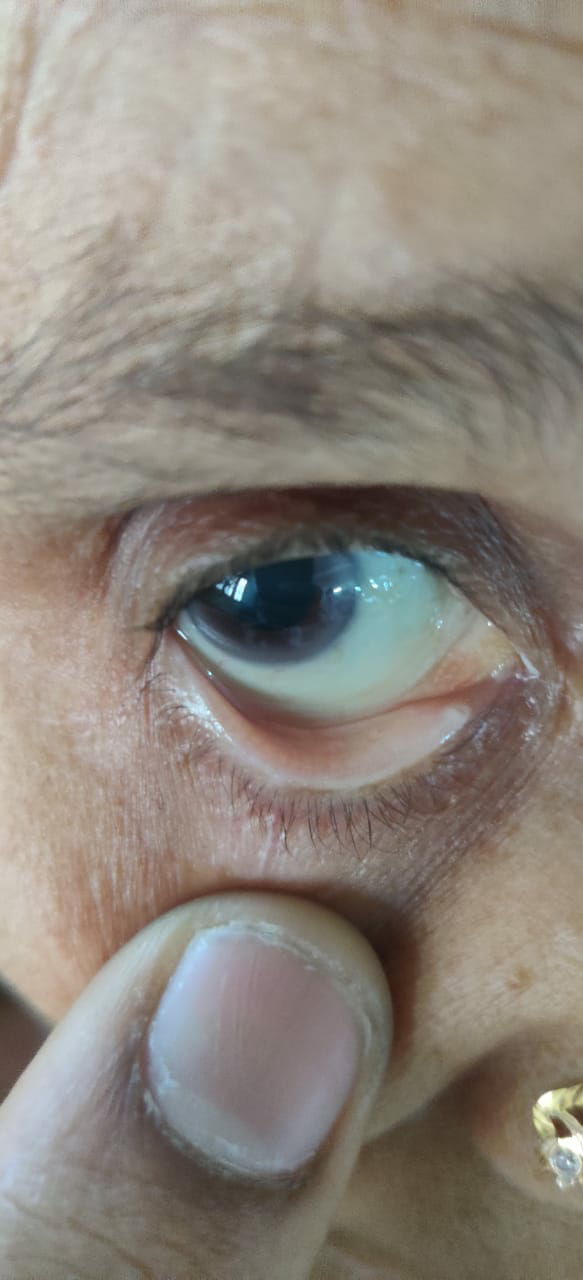
1.)I've seen a case of 37/M with hronic decompensated liver disease secondary to alcoholism which was admitted under our unit.Patient had ascites (shifting dullness+,b/l flanks-dull note).
Ascitic tap was done for our patient


3.) Learnt how to take ABG samples from radial and brachial arteries.
4.) Performed high quality CPR.
5.) Seen a case of Right facio brachial monoparesis with acute infarct in left frontal lobe with early hemorrhagic reperfusion injury.
6.) Seen case of Right upper lobe fibrosis and learnt management.
7.) Seen cases of hypertensive emergency and followed up.